Introduction
Apophysial avulsion fractures of the pelvis are rare injuries that affect young athletes. They typically occur during sudden strong muscle contraction due to weakness of the growth cartilage [1, 2]. Today, adolescent sportive injuries are becoming a major problem with their increasing frequency and importance. The connection between the apophysis and the body of the bone becomes stronger, after the ossification at growth cartilage and the weakest structure in transferring force between muscle and bone becomes the musculotendinous junction [3]. These injuries mostly occur in competitive sports, with sudden changes in direction during hitting, running and sprinting. In a study, the most common injuries were spina iliac anterior inferior (SIAI) avulsion (46 %), followed by spina iliac anterior superior (SIAS) avulsion (32 %), ischial tuberocyte (IT) avulsion (12 %) and iliac crest (IK) avulsion (11 %) [4]. The patient's medical history, detailed physical examination and imaging methods are used in the diagnosis. Treatment methods include conservative and surgical treatment options.
Case Reports
This is a retrospective case series of two patients with SIAI avulsion fractures that were treated surgically after failed conservative treatment and one patient with a SIAS avulsion fracture who was treated with immediate surgery. Common complaints were sudden onset of groin pain that caused limping. All patients were amateur adolescent football players. Their age was 13, 15 and 16 (mean 14.6) and they were all male.
Cases 1 and 2: 13 and 15 years old male patients were presented with complaints of inguinal pain and inability to return to sports activities for 1.5 years and 7 months. Both patients could not continue the game with sudden inguinal pain after hitting the ball during a football match. Conservative treatment was applied, but they had to quit football due to continious pain. Both patients had groin pain during running and strenuous activities, they had full range of motion of the hip joints, but hip pain in 90 degree hip flexion and internal rotation. Hip impingement tests of both patients were positive.
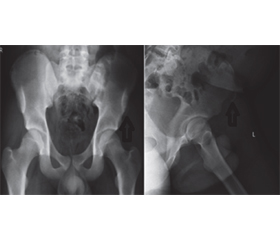
After comprehensive evaluation, the diagnosis of SIAI avulsion fracture was made (fig. 1, 3). It was concluded that there was femoroacetabular impingement as a result of heterotopic ossification of the SIAI avulsion fracture. Nonsteroidal anti-inflammatory drugs and rehabilitation were initiated in the patients. They were followed up for 3 months, but the complaints of the patients did not regress and surgical treatment was decided. Surgical excision of the heterotopic osseöz tissue was performed in both patients using the Smith-Petersen approach (fig. 2, 4). There were no complications in the postoperative period. Physiotherapy in the form of range of motion and strengthening exercises was started 3 weeks later. In their 6-week follow-up, their hip examinations were painless, they had full range of motion, and impingement tests were negative. Both patients returned to full sportive activities after 6 months.
/69.jpg)
Case 3: a 16-year-old male patient fell down due to a sudden pain in his left groin while running during warming up before the match and the patient was brought to emergency department afterwards. His left hip joint range of motion was decreased in his initial physical examination. Pain in hip flexion and internal rotation, and crepitation on the left SIAS were observed. A diagnosis of left SIAS avulsion fracture was made with X-ray and CT images (fig. 5). Surgical treatment was applied on the third day of the trauma. The avulsed part was approached with a 5 cm vertical incision and it was fixed with two cannulated screws (fig. 6). There were no postoperative complications. Partial weight bearing was allowed and active hip flexion was prohibited after the operation. Rehabilitation started after the second week. The patient’s follow-up continues.
Discussion
Adolescent pelvic avulsion fractures are rare injuries that can be missed easily and their incidence is increasing due to the increase in adolescent sportive activities [5, 6]. The literature is still controversial about the choice of treatment whether surgery or conservative. Early diagnosis is essential to ensure appropriate treatment. Patients with typical clinical findings and a history of trauma should have at least bilateral pelvic radiography and CT if necessary. MRI or ultrasound can be used to see a possible soft tissue injury [7, 8].
There are conservative and surgical methods in the treatment of pelvic apophyseal avulsion fractures. Since the periosteum is relatively thicker in adolescents, conservative treatment with an appropriate rehabilitation program is the preferred treatment method for non-displaced fractures [2, 9].
Conservative treatment with analgesics, limited activities, and partial weight on crutches for at least 3–6 weeks has been shown to be successful in most of these injuries [9, 10]. Metzmaker et al. presented the successful nonoperative management of 27 avulsion fractures using a staged rehabilitation protocol with full return to sport up to 2 months after injury [9].
Potential complications of conservative therapy include nonunion or heterotopic ossification, shortening of the origin of the hamstrings, and “hamstring syndrome” in which fibrosis develops [7]. These complications may be associated with chronic pain at the former fracture site and a significant reduction in sportive ability [10]. Heterotopic ossification, which causes symptomatic hip compression and incessant pain, indicates a failure of nonoperative therapy and requires operative intervention [11].
In series, two patients were treated conservatively for SIAI avulsion fractures but pain and signs of impingement were permanent. Metzmaker et al. demonstrated the success of nonoperative treatment with an appropriate rehabilitation program [9]. We think that these patients did not receive appropriate rehabilitation. Although conservative treatment was also tried appropriotely in one patient in our clinic, the complaints of the patient did not decrease. Heterotophic ossification was also observed in the patients. Two patients were operated with the same surgical method and ossification was excised. Pathology reports were also compatible with our definition. In the follow-up of the patients, it was observed that the complaints were completely resolved, there were no impingement signs and they had full range of motion.
A meta-analysis involving 596 patients showed superior results with operative treatment. Return to sports was 92 % in operatively treated patients and 80 % in nonoperatively treated patients, the fractures which were displaced more than 15 mm and elite athletes are candidates for surgical treatment [11].
One patient who was an amateur football player, had a sudden onset of severe pain in his left hip during warm up before the football match and underwent surgery with the diagnosis of avulsion fracture in SIAS. Surgical treatment was planned to start sportive activities earlier. Open reduction was made and the avulsion fracture was fixed with cannulated screws. This patient has been operated recently and the follow-up period is only three weeks. His follow-up continues.
Conclusions
In conclusion, pelvic apophysis avulsion fractures in adolescents are rare but important injuries and mostly seen in athletes. Conservative treatment and surgical treatment are among the treatment methods. Complications that may occur after inappropriate conservative treatment (impingement due to heterotophic ossification) that delay the return of sportive activities. Appropriate treatment should be chosen for early return to sportive activities.
Received 19.03.2021
Revised 30.03.2021
Accepted 05.04.2021
Список литературы
1. Howard F.M., Piha R.J. Apophysis fractures in adolescent athletes. JAMA. 1965. 192. 842-844. [PubMed] [Google Scholar]
2. McKinney B.I., Nelson C., Carrion W. Apophyseal avulsion fractures of the hip and pelvis. Orthopedics. 2009. 32. 42-48. [PubMed] [Google Scholar]
3. Porr J., Lucaciu C., Birkett S. Avulsion fractures of the pelvis — a qualitative systematic review of the literature.
J. Can. Chiropr. Assoc. 2011. 55. 247-255. [PMC free article] [PubMed] [Google Scholar]
4. Calderazzi F., Nosenzo A., Galavotti C., Menozzi M., Pogliacomi F., Ceccarelli F. Apophyseal avulsion fractures of the pelvis. A review. Acta Biomed. 2018. 89. 470-476. [PMC free article] [PubMed] [Google Scholar]
5. Biedert R.M. Surgical treatment of traumatic avulsion of ischial tuberosity in young athletes. Clin. J. Sport Med. 2015. 25. 67-72. doi: 10.1097/JSM.0000000000000088. [PubMed] [CrossRef] [Google Scholar]
6. Schuett D.J., Bomar J.D., Pennock A.T. Pelvic apophyseal avulsion fractures: a retrospective review of 228 ca-ses. J. Pediatr. Orthop. 2015. 35. 617-623. doi: 10.1097/BPO.0000000000000328. [PubMed] [CrossRef] [Google Scholar]
7. Ferlic P.W., Sadoghi P., Singer G., Kraus T., Eberl R. Treatment of ischial tuberositic avulsion fractures in adolescent athletes. Knee Surgery Sports Traumatol Arthrosc. 2013. 22. 893-897. doi: 10.1007/s00167-013-2570-4. [PubMed] [CrossRef] [Google Scholar]
8. Gidwani S., Bircher M.D. Hamstring-induced avulsion injuries — a set of 12 patients and their management algorithm. Ann. R. Coll. Surg. Engl. 2007. 89. 394-399. doi: 10.1308/003588407X183427. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
9. Metzmaker J.N., Pappas A.M. Avulsion fractures of the pelvis. J. Sports Med. 1985. 13. 349-358. doi: 10.1177/
036354658501300510. [PubMed] [CrossRef] [Google Scholar]
10. Linni K., Mayr J., Höllwarth M.E. Minor apophysis fractures of the pelvis and trochanter in 20 adolescents and 2 young children. Unfallchirurg. 2000. 103. 961-964. doi: 10.1007/s001130050653. [PubMed] [CrossRef] [Google Scholar]
11. Larson C.M., Kelly B.Y., Stone R.M. Constructing a case for anterior lower iliac spine/subvertebral hip compression: three representative case reports and proposed concept. Arthroscopy. 2011. 27(12). 1732-1737. doi: 10.1016/j.arthro.2011.10.004. [PubMed] [CrossRef] [Google Scholar]

/69.jpg)
/70.jpg)