
Журнал «Здоровье ребенка» Том 20, №7, 2025
Вернуться к номеру
Рівні гемоглобіну та IL-6 у дітей із затримкою росту і туберкульозною інфекцією, які отримують пероральні харчові добавки: дослідження з одногруповим дизайном і аналізом до та після втручання
Авторы: Marisa Tulus Purnomo, Nur Aisiyah Widjaja, Retno Asih Setyoningrum
Faculty of Medicine, Universitas Airlangga, Soetomo General Academic Hospital, Surabaya, Indonesia
Рубрики: Педиатрия/Неонатология
Разделы: Клинические исследования
Версия для печати
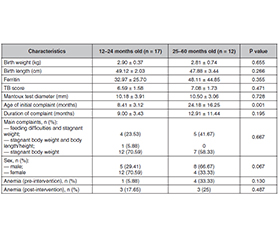
Актуальність. Недоїдання, спричинене туберкульозом, часто зустрічається в дітей і супроводжується дефіцитом мікроелементів через нестачу поживних речовин, зокрема залізодефіцитною анемією. Недоїдання також викликає зниження рівня інтерлейкіну (IL)-6, що робить дітей вразливими до інфекції. Мета: проаналізувати вплив пероральних харчових добавок на рівень гемоглобіну (Hb), IL-6, приріст маси й довжини тіла в дітей із затримкою росту і туберкульозом. Матеріали та методи. Преекспериментальне дослідження з одногруповим дизайном і аналізом до та після втручання проводилося з жовтня 2022 року до липня 2023 року в приватній лікарні м. Сурабая (Східна Ява, Індонезія) за участю дітей віком від 12 до 60 місяців із затримкою росту й туберкульозною інфекцією. Статистичний аналіз включав описову статистику (середнє значення ± стандартне відхилення або n (%)), T-критерій для незалежної вибірки або U-критерій Манна — Вітні, а також T-критерій парних вибірок або критерій рангових знаків Вілкоксона залежно від нормальності розподілу. Результати. У дослідженні взяли участь 29 дітей, середній вік яких становив 25,40 ± 11,30 місяця. 58,62 % пацієнтів були віком до 24 місяців, а 41,38 % — від 25 до 60 місяців. Суттєвої різниці в рівнях IL-6 та Hb до та після втручання не спостерігалося. Середній уміст Hb на початку дослідження становив 12,07 ± 1,22 мг/дл, після — 12,00 ± 1,09 мг/дл, тоді як для IL-6 ці показники дорівнювали відповідно 125,76 ± 116,87 мкг/л та 122,41 ± 104,43 мкг/л (p = 0,441). Висновки. Прийом пероральних харчових добавок протягом 90 днів не вплинув на рівень IL-6 та Hb в дітей із туберкульозом.
Background. Undernutrition due to tuberculosis (TB) infection is high in children and is often accompanied by micronutrient deficiency resulting from insufficient nutritional intake such as iron deficiency anemia. Undernutrition also caused a decrease in IL-6, making children vulnerable to the infection. This study was aimed at analyzing the effect of oral nutritional supplements on hemoglobin, interleukin (IL)-6 levels, weight and length increment in stunted children with TB. Materials and methods. A pre-experimental study with one-group pre-test/post-test design was conducted from October 2022 to July 2023 in a private hospital, Surabaya, East Java, involving stunted children with TB infection aged 12 to 60 months. The statistical analysis included descriptive statistics (mean ± standard deviation or n (%)), independent sample T-test or Mann-Whitney U test, and paired sample T-test or Wilcoxon sign rank test, depending on the normality. Results. A total of 29 subjects were enrolled in this study, with a mean age of 25.40 ± 11.30 months. 58.62 % of subjects were aged below 24 months old, and 41.38 % were aged between 25 and 60 months. No significant differenсе was seen in IL-6 and hemoglobin before and after the intervention. The average hemoglobin level before the intervention was 12.07 ± 1.22 mg/dL, and after the intervention it was 12.00 ± 1.09 mg/dL, while for IL-6, these indicators were 125.76 ± 116.87 and 122.41 ± 104.43 µg/L, respectively (p = 0.441). Conclusions. Oral nutritional supplements intervention for 90 days did not affect IL-6 and hemoglobin levels of children with TB.
туберкульоз; затримка росту; інтерлейкін-6; анемія; гемоглобін
tuberculosis; stunted growth; IL-6; anemia; hemoglobin
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Soliman A, De Sanctis V, Alaaraj N, et al. Early and long-term consequences of nutritional stunting: from childhood to adulthood. Acta Biomed. 2021;92:1-12.
- Wicaksono RA, Arto KS, Mutiara E, et al. Paediatrica Indonesiana. Paediatr Indones. 2021;61:12-19.
- Bustami B, Ampera M. The identification of modeling causes of stunting children aged 2–5 years in Aceh province, Indonesia (data analysis of nutritional status monitoring 2015). Open Access Maced J Med Sci. 2020;8:657-663.
- Marlina H, Triana A, Fanora E. Causes of stunting in toddlers: literature review. Int J Multidiscip Res Growth Eval. 2022;138-142.
- Permatasari DF, Sumarmi S. Differences of born body length, history of infectious diseases, and development between stunting and non-stunting toddlers. J Berk Epidemiol. 2018;6:182.
- Ait-Khaled N, Enarson DA. Tuberculosis: a manual for medical students. Geneva, Switzerland: WHO; 2005.
- World Health Organization (WHO). Global tuberculosis report: executive summary 2020. Geneva, Switzerland: WHO; 2020.
- Jaganath D, Mupere E. Childhood tuberculosis and malnutrition. J Infect Dis. 2012;206:1809-1815.
- Padmapriyadarsini C, Shobana M, Lakshmi M, et al. Undernutrition and tuberculosis in India: situation analysis and the way forward. Indian J Med Res. 2016;144:11-20.
- Gwela A, Mupere E, Berkley JA, et al. Undernutrition, host immunity and vulnerability to infection among young children. Pediatr Infect Dis J. 2019;38:e175-e177.
- Hossain M, Nahar B, Haque MA, et al. Serum adipokines, growth factors, and cytokines are independently associated with stunting in Bangladeshi children. Nutrients. 2019;11:1827.
- Mohseni M, Ahmadi S, Asadi H, et al. A systematic review and meta-analysis of the prevalence of malnutrition among 6–14-year-old children in Iran. Int J Prev Med. 2022;13:138.
- Alaaraj N, Soliman A, Rogol AD. Growth of malnourished infants and children: how is inflammation involved? Expert Rev Endocrinol Metab. 2021;16:213-216.
- Holt LE, Snyderman SE. Protein and amino acid requirements of infants and children. Nutr Abstr Rev. 1965;35:1-13.
- Philipson TJ, Snider JT, Lakdawalla DN, et al. Impact of oral nutritional supplementation on hospital outcomes. Am J Manag Care. 2013;19:121-128.
- Pham DT, Ninh NT, Hoang TN, et al. The effectiveness of oral nutritional supplements improves the micronutrient deficiency of Vietna–mese children with stunting. Arch Pharm Pract. 2020;11:7-13.
- Uí Dhuibhir P, Collura N, Walsh D. Complete oral nutritional supplements: dietitian preferences and clinical practice. J Diet Suppl. 2019;16:40-50.
- Collins C, Tucker C, Walton C, et al. Pharmacy technician review of oral nutritional supplements (ONS) within care homes. Pharmacy. 2019;7:28.
- Yeung SSY, Lee JSW, Kwok T. A nutritionally complete oral nutritional supplement powder improved nutritional outcomes in free-living adults at risk of malnutrition: a randomized controlled trial. Int J Environ Res Public Health. 2022;19. doi: 10.3390/ijerph191811354.
- Thomas TA. Tuberculosis in children. Pediatr Clin North Am. 2018;64:893-909.
- Tadesse F, Mitiku H, Girma S, et al. Magnitude of undernutrition and associated factors among adult tuberculosis patients attending public health facilities in Haramaya District, Eastern Ethiopia. BMC Pulm Med. 2023;23:42.
- Wassie EG, Tenagashaw MW, Tiruye TY. Women empowerment and childhood stunting: evidence from rural northwest Ethiopia. BMC Pediatr. 2024;24:30.
- Karki A. Prevalence and determinants of stunting among children under 5 years in remote Nepal. Reprod Female Child Heal. 2023;2:233-241.
- Laksono AD, Wulandari RD, Amaliah N, et al. Stunting among children under two years in Indonesia: does maternal education matter? PLoS One. 2022;17:1-11.
- Téllez-Navarrete NA, Ramón-Luing LA, Muñoz-Torric M, et al. Malnutrition and tuberculosis: the gap between basic research and clinical trials. J Infect Dev Ctries. 2021;15:310-319.
- Gao Z, Liu Q, Deng Q, et al. Growth and anemia among children with tuberculosis infection at different sites in Southwest China. Front Pediatr. 2023;11:1-9.
- Maseko TG, Ngubane S, Letsoalo M, et al. Higher plasma interleukin-6 levels are associated with lung cavitation in drug-resistant tuberculosis. BMC Immunol. 2023;24:26.
- Ren Z, Zhao F, Chen H, et al. Nutritional intakes and associated factors among tuberculosis patients: a cross-sectional study in China. BMC Infect Dis. 2019;19:1-8.
- Mithra P, Khatib MN, Sinha AP, et al. Interventions for addressing anemia among children and adolescents: an overview of systematic reviews. Front Pediatr. 2021;8:549549.
- Martinez L, Gray DM, Botha M, et al. The long-term impact of early-life tuberculosis disease on child health. Am J Respir Crit Care Med. 2023;207:1080-1088.
- Chaparro CM, Suchdev PS, Nutrition I. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann NY Acad Sci. 2019;1450:15-31.
- Boni FG, Hamdi I, Koundi LM, et al. Cytokine storm in tuberculosis and IL-6 involvement. Infect Genet Evol. 2022;97. doi: 10.1016/j.meegid.2021.105166.
- Vita G, Syambani Z. Interleukin-6 levels in children developing SARS-CoV-2 infection. Pediatr Neonatol. 2020;61:253-254.
- Wang Y, Wang L, Wen Z, et al. High IL-6 and –VEGF-A levels correlate with delayed wound healing in cervical lymph node tuberculosis patients. Int J Tuberc Lung Dis. 2018;22:1227-1232.
- Vivekanandan MM, Adankwah E, Aniagyei W, et al. Plasma cytokine levels characterize disease pathogenesis and treatment response in tuberculosis patients. Infection. 2023;51:169-179.
- Succurro E, Andreozzi F, Sciaqua A, et al. Reciprocal association of plasma IGF-1 and interleukin-6 levels with cardiometabolic risk factors in nondiabetic subjects. Diabetes Care. 2008;31:1886-1888.
- Redford P, Murray P, O’Garra A. The role of IL-10 in immune regulation during M. tuberculosis infection. Mucosal Immunol. 2011;4:261-270.
- Fâcă AI, Udeanu DI, Arsene AL, et al. Nutritional deficiencies and management in tuberculosis: pharmacotherapeutic and clinical implications. Nutrients. 2025;17:1878.