
Журнал «Медицина неотложных состояний» Том 21, №7, 2025
Вернуться к номеру
Оцінка ефективності шкали тяжкості сепсису WSES у прогнозуванні наслідків внутрішньочеревних інфекцій
Авторы: Khalid Khairi Hussein
College of Medicine, Tikrit University, Iraq
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
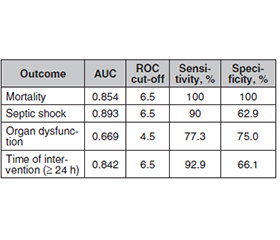
Актуальність. Внутрішньочеревні інфекції (ВЧІ) є основною причиною захворюваності та смертності. Шкала тяжкості сепсису Всесвітнього товариства невідкладної хірургії (WSES) виявилася корисною в прогнозуванні результатів лікування у критично хворих пацієнтів із ВЧІ. Мета: визначити цінність шкали WSES у прогнозуванні смертності, септичного шоку, органної дисфункції та затримки хірургічного втручання в осіб із ВЧІ. Матеріали та методи. Проспективне когортне дослідження проводилося в навчальній лікарні Тікрита (Ірак) з жовтня 2023 року по червень 2024 року за участю 91 пацієнта з ВЧІ. Було оцінено демографічні дані, джерела інфекції, показники за шкалою WSES та клінічні результати. Прогностичну цінність шкали WSES щодо смертності, септичного шоку, органної дисфункції та затримки втручання визначали за допомогою ROC-кривої. Результати. Серед обстежених 63,74 % становили чоловіки, а 37,78 % осіб були віком понад 70 років. Найпоширенішими джерелами інфекції були перфорація апендикса (38,89 %), відкрита виразка дванадцятипалої кишки (21,11 %) та недивертикулярна перфорація товстої кишки (20 %). Шкала WSES продемонструвала високу прогностичну цінність щодо клінічних результатів. Площа під кривою (AUC) для смертності становила 0,854, з ідеальною чутливістю та специфічністю при пороговому значенні 6,5. Для септичного шоку AUC дорівнювала 0,893, з чутливістю 90 % та специфічністю 62,9 %. Шкала WSES також була корисною в прогнозуванні органної дисфункції (AUC 0,669) та затримки втручання (AUC 0,842). Логістичний регресійний аналіз показав, що вищі бали за шкалою WSES вірогідно підвищують ризик смертності (відношення шансів (ВШ) 2,060), септичного шоку (ВШ 2,108) та органної дисфункції (ВШ 2,214). Висновки. Шкала тяжкості сепсису WSES є високоефективним інструментом для прогнозування критичних результатів у пацієнтів із внутрішньочеревними інфекціями. Можливість прогнозувати смертність, септичний шок та затримку втручання підкреслює її корисність щодо прийняття клінічних рішень, особливо в пацієнтів із високим ризиком. Стратифікація за шкалою WSES вимагає своєчасного втручання для поліпшення результатів лікування цієї групи хворих.
Background. Intra-abdominal infections (IAIs) are a major cause of morbidity and mortality. The World Society of Emergency Surgery (WSES) Sepsis Severity Score has been found to be useful in predicting the outcomes of critically ill patients with IAIs. The objective of this study was to determine the value of the WSES score in predicting mortality, septic shock, organ dysfunction and delayed surgical intervention in patients with IAIs. Materials and methods. The prospective cohort study took place at Tikrit Teaching Hospital from October 2023 through June 2024. The research included 91 patients who suffered from IAIs. Demographic data, infection sources, WSES scores and clinical outcomes were recorded. The predictive value of the WSES score for mortality, septic shock, organ dysfunction and delayed intervention was assessed using a receiver operating characteristic (ROC) curve. Results. Among the cohort, 63.74 % were male, and 37.78 % were over 70 years old. The most common sources of infection were perforated appendix (38.89 %), perforated duodenal ulcer (21.11 %), and non-diverticular colonic perforation (20 %). The WSES score demonstrated a strong predictive value for outcomes. The area under the curve (AUC) for mortality was 0.854, with perfect sensitivity and specificity at a cutoff of 6.5. For septic shock, the AUC was 0.893, with a sensitivity of 90 % and specificity of 62.9 %. The WSES score was also predictive of organ dysfunction (AUC 0.669) and delays in intervention (AUC 0.842). Logistic regression analysis revealed that higher WSES scores significantly increased the odds of mortality (odds ratio (OR) 2.060), septic shock (OR 2.108), and organ dysfunction (OR 2.214). Conclusions. The WSES Sepsis Severity Score is a highly effective tool for predicting critical outcomes in patients with intra-abdominal infections. Its ability to forecast mortality, septic shock, and delays in intervention underscores its utility in guiding clinical decision-making, particularly in high-risk patients. The WSES score stratification demands prompt intervention to improve treatment outcomes for this patient group.
внутрішньочеревні інфекції; шкала тяжкості сепсису; Всесвітнє товариство невідкладної хірургії; прогнозування смертності; септичний шок
intra-abdominal infections; Sepsis Severity Score; World Society of Emergency Surgery; mortality prediction; septic shock
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Tish S, Corcelles R. The art of sleeve gastrectomy. J Clin Med. 2024;13(7):1954. doi: 10.3390/jcm13071954.
- Menichetti F, Sganga G. Definition and classification of intra-abdominal infections. J Chemother. 2009;21(suppl 1):3-4.
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323-9. doi: 10.1179/joc.2009.21.
- Wacha H, Linder MM, Feldman U, Wesch G, Gundlach E, Steifensand RA. Mannheim peritonitis index (prediction of risk of death from peritonitis: construction of a statistical and validation of an empirically based index). Theoretical Surg. 1987;1:169-77.
- Qureshi AM, Zafar A, Saeed K, Quddus A. Predictive po–wer of Mannheim Peritonitis Index. J Coll Physicians Surg Pak. 2005;15(11):693-6.
- Budzyski P, Dworak J, Natkaniec M, Pdziwiatr M, Major P, Migaczewski M, et al. The usefulness of the Mannheim Peritonitis index score in assessing the condition of patients treated for peritonitis. Pol Przegl Chir. 2015;87(6):301-6. doi: 10.1515/pjs-2015-0058.
- Sartelli M, Abu-Zidan FM, Catena F, Griffiths EA, Di Saverio S, et al. Global validation of the WSES Sepsis Severity Score for patients with complicated intra-abdominal infections: a prospective multicentre study (WISS Study). World J Emerg Surg. 2015;10:61.
- Mwenda KI, Ojuka D, Awori M. Utility of World Society of Emergency Surgery Sepsis Severity Score in predic–ting outcomes of intra-abdominal infections. Ann Afr Surg. 2020;17(2):65-8.
- Godnez-Vidal AR, Vzquez-Rentera R, Guerrero-Ponce AE, et al. Use of the WSES scale to predict mortality in patients with intra-abdominal infection. Rev Mex Cir Aparato Dig. 2020;9(2):65-70.
- Bone RC, Baulk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101(6):1644-55.
- Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens Y-E, Avondo A, et al. Prognostic accuracy of Sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA. 2017;317(3):301-8.
- Osatnik J, Tort-Oribea B, Folco J, et al. Predictive performance of Quick Sequential Organ Failure Assessment Scoring in an Argentinian hospital. J Clin Diagn Res. 2018;12(10):22-6.
- Wabwire B, Saidi H. Stratified outcome evaluation of peritonitis. Ann Afr Surg. 2014;11(2):29-34.
- Green S, Kong V, Clarke D, et al. The spectrum and outcome of surgical sepsis in Pietermaritzburg, South Africa. S Afr Med J. 2017;107(2):134-6.
- Parlato M, Philippart F, Rouquette A, et al. Circulating biomarkers may be unable to detect infection at the early phase of sepsis in ICU patients: the CAPTAIN prospective multicenter cohort study. Intensive Care Med. 2018;44:1061-70. doi: 10.1007/s00134-018-5228-3.
- Weiss SL, Peters MJ, Alhazzani W, Agus MS, Flori HR, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction. Intensive Care Med. 2020;46:10-67.
- Asner SA, Desgranges F, Schrijver IT, Calandra T. Impact of the timeliness of antibiotic therapy on the outcome of patients with sepsis and septic shock. J Infect. 2021;82(5):125-34.
- Santucci C, Carioli G, Bertuccio P, Malvezzi M, Pastorino U, et al. Progress in cancer mortality, incidence, and survival: a global overview. Eur J Cancer Prev. 2020;29(5):367-81.
- Dimitrov E, Minkov G, Enchev E, Yovtchev Y. The World Society of Emergency Surgery Sepsis Severity Score shows no prognostic superiority over the Mannheim Peritonitis Index in patients with complicated intra-abdominal infections. J Emerg Med Trauma Acute Care. 2022;2022(4):24. doi: 10.5339/jemtac.2022.24.
- Dellinger RP, Rhodes A, Evans L, Alhazzani W, Beale R, et al. Surviving sepsis campaign. Crit Care Med. 2023;51(4):431-44.