
Международный неврологический журнал Том 21, №6, 2025
Вернуться к номеру
Роль триптанів у сучасних підходах до абортивного лікування мігрені
Авторы: Боженко М.І.
ДНП «Львівський національний медичний університет імені Данила Галицького», м. Львів, Україна
Рубрики: Неврология
Разделы: Справочник специалиста
Версия для печати
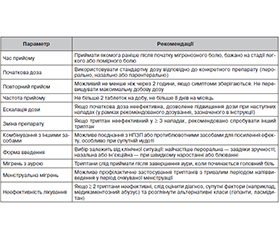
Ще кілька десятиліть тому можливості фармакологічного лікування мігрені були вкрай обмеженими, що знижувало ефективність контролю симптомів у більшості пацієнтів. Проте останні роки ознаменувалися суттєвим прогресом у розумінні патофізіології мігрені та розвитку нових терапевтичних підходів. Враховуючи появу нових препаратів, багаторічне накопичення досвіду використання інших препаратів, важливо зрозуміти, яке місце займають триптани в сучасному абортивному лікуванні мігрені. Мета статті: проаналізувати роль триптанів у сучасному абортивному лікуванні мігрені. Ця стаття підготовлена у форматі наративного огляду. Пошук літератури проводився у базах даних PubMed, Scopus та Web of Science. До аналізу були включені статті, опубліковані в період з 2015 до 2025 року. Перевага надавалася клінічним настановам, систематичним оглядам, метааналізам, рандомізованим контрольованим дослідженням та великим обсерваційним роботам. Огляд літератури та обговорення. Одним з ключових кроків у лікуванні мігрені, який є необхідним для кожного пацієнта — підбір якісного абортивного лікування. Виділяють 2 основних підходи до абортивного лікування мігрені — стратифікований підхід та поетапний підхід. В умовах спеціалізованої допомоги доцільніше застосовувати стратифікований підхід, при якому вибір терапії залежить від тяжкості нападу та індивідуальних потреб і особливостей пацієнта. На сьогодні порівняння між препаратами для абортивного лікування мігрені значною мірою базується на систематичних оглядах та мережевих метааналізах. Під час аналізу таких робіт бачимо, що є багато активних препаратів, які демонструють свою ефективність порівняно з плацебо для досягнення знеболювання через 2 години. Найефективнішими серед них є триптани. При цьому найвищу ефективність серед триптанів продемонстрував елетриптан. Нові препарати, як-от ласмідитан, рімегепант і уброгепант, демонструють нижчу ефективність порівняно з триптанами. Але при цьому у пацієнтів, які недостатньо реагують на триптани, вони можуть бути ефективними. Проте слід враховувати також побічні ефекти і профіль безпеки препаратів. Тут гепанти і НПЗП мають перевагу над триптанами і дитанами. Для досягнення оптимального ефекту від прийому триптанів і мінімізації побічних ефектів важливо дотримуватися правил їх прийому. Також потрібно враховувати ціну препаратів та її співвідношення з ефективністю. Є суттєва різниця в ціні між новими препаратами та триптанами в європейських країнах та в США. Висновки. Останніми роками з’явилися нові препарати для абортивного лікування мігрені, що розширює можливості більш персоніфікованого підходу до лікування. Триптани залишаються найефективнішими ліками для зняття та полегшення нападів мігрені. Водночас гепанти стають новою можливістю для пацієнтів, які не реагують на триптани або погано толерують їх побічні ефекти. При персоніфікованому підході до вибору абортивної терапії також слід враховувати значно нижчу ціну триптанів порівняно з новими препаратами.
Several decades ago, pharmacological options for the treatment of migraine were extremely limited, reducing ability to effectively control symptoms in most patients. In recent years, significant advances have been made in understanding migraine pathophysiology and in the development of novel therapeutic approaches. Given the emergence of new drugs alongside long-standing clinical experience with established treatments, it is important to clarify the role of triptans in contemporary acute migraine management. Aim purpose of this article was to analyze the role of triptans in modern acute migraine therapy. Methods. This narrative review was conducted through systematic searches of PubMed, Scopus, and Web of Science. Articles published between 2015 and 2025 were included, with preference given to clinical guidelines, systematic reviews, meta-analyses, randomized controlled trials, and large observational studies. Literature Review and Discussion. Selecting an effective acute therapy is a critical step in migraine management for every patient. Two main strategies are recognized: the stratified approach and the escalating approach. In specialized care settings, a stratified approach — tailored to attack severity and individual patient characteristics — is generally preferred. Today, comparative efficacy among acute migraine therapies is largely based on systematic reviews and network meta-analyses. Numerous active agents demonstrate significant benefit over placebo in achieving pain relief at two hours, with triptans consistently showing the highest efficacy. Among triptans, eletriptan has demonstrated superior effectiveness. Novel agents, including lasmiditan, rimegepant, and ubrogepant, show comparatively lower efficacy but they may be valuable for patients who respond insufficiently to triptans. However, side effects and safety profile are also critical: gepants and nonsteroidal anti-inflammatory drugs exhibit advantages over triptans and ditans. Optimal use of triptans requires adherence to administration guidelines to maximize efficacy and minimize side effects. Cost-effectiveness should also be considered, as substantial price differences exist between newer agents and triptans across Europe and the United States. Conclusions. Recently, the introduction of new acute migraine therapies expands opportunities for personalized treatment. Triptans remain the most effective agents for aborting and relieving migraine attacks, whereas gepants offer alternative option for patients with inadequate response or poor tolerability to triptans. When individualizing acute therapy, the markedly lower cost of triptans compared to novel agents should be factored into clinical decision-making.
мігрень; лікування; триптани; біль
migraine; treatment; triptans; pain