
Архів офтальмології та щелепно-лицевої хірургії України Том 2, №1, 2025
Вернуться к номеру
Вплив позиціонування малогомілкового клаптя на біомеханічні властивості протезних конструкцій з опорою на дентальні імплантати у пацієнтів із сегментарними дефектами нижньої щелепи
Авторы: Філоненко Д.О. (1), Чепурний Ю.В. (1), Крищук М.Г. (2), Копчак А.В. (1)
(1) - Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
(2) - Національний технічний університет України «Київський політехнічний інститут імені Ігоря Сікорського», м. Київ, Україна
Рубрики: Хирургия, Офтальмология
Разделы: Клинические исследования
Версия для печати
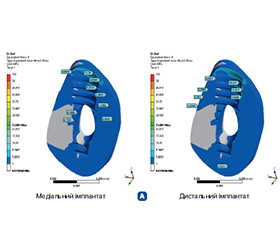
Актуальність. Дефекти нижньої щелепи можуть утворюватися після оперативного втручання внаслідок пухлинного процесу, а також бути наслідком вогнепальних поранень щелепно-лицевої ділянки. Ефективним з клінічної точки зору та очевидним з позицій вибору є застосування васкуляризованих комбінованих клаптів з малогомілкової кістки. Позиціонування кісткового трансплантату відносно збереженої частини нижньої щелепи визначає можливості подальшого встановлення дентальних імплантатів та якісного протетичного лікування. Проте кожна з позицій фіксації має свої переваги та недоліки. Мета: вивчити в модельному експерименті особливості напружено-деформованого стану кісткової тканини вільного трансплантату з малогомілкової кістки, що заміщує сегментарний дефект щелепи. Матеріали та методи. Було використано метод імітаційного комп’ютерного моделювання напружено-деформованого стану нижньої щелепи із заміщеними в різний спосіб сегментарними дефектами після протетичної реабілітації хворих незнімними конструкціями із опорою на дентальні імплантати. Загалом було згенеровано й обчислено 4 моделі, що відтворювали 2 типи геометрії і 2 типи навантаження. Результати. У кістковій тканині напруження концентрувалися навколо перших 2–3 витків різьби із максимальними значеннями навколо першого витка. У самому імплантаті напруження зосередились на ділянці абатменту. Виявлено, що в умовах вертикального та горизонтального навантаження, яке відповідає змиканню зубів за фізіологічних умов жувального навантаження, розташування малогомілкового трансплантату в ділянці основи альвеолярного відростка було асоційовано зі зменшенням максимальних значень еквівалентних напружень за Мізесом в імплантатах на 16–63 %. У кістковій тканині редукція навантаження відбулася на 30–53 % порівняно з моделлю, у якій кістковий трансплантат був розташований вздовж нижнього краю щелепи. Висновки. При більш високому розташуванні кісткового компонента малогомілкового клаптя виникали адекватні умови напружено-деформованого стану та нормальний розподіл локальних навантажень, що, очевидно, визначає кращий прогноз остеоінтеграції, виживаності та функціонування дентальних імплантатів.
Background. Defects of the lower jaw can be formed after surgery due to a tumor process and also be the result of gunshot wounds to the maxillofacial area. The use of vascularized combined fibula flaps is clinically effective and obvious from the standpoint of choice. The positioning of the bone graft relative to the preserved part of the lower jaw determines the option for further dental implant procedure and high-quality prosthetic treatment. However, each of the fixation positions has its advantages and disadvantages. The goal is to study the peculiarities of the stress-strain state of bone tissue of a fibula free flap that replaces a segmental defect of the jaw in a model experiment. Materials and methods. The method of simulation computer modeling of the stress-strain state of the lower jaw with segmental defects replaced in different ways after the prosthetic rehabilitation of patients with fixed structures supported on dental implants was used. In total, 4 models were generated and calculated, reproducing 2 types of geometry and 2 types of loading. Results. In bone tissue, stresses were concentrated around the first 2–3 turns of the thread with maximum values around the first turn. In the implant itself, the stresses were concentrated in the area of the abutment. It was found that under conditions of vertical and horizontal loading, which corresponds to the occlusion under physiological conditions of chewing load, the location of the fibula flap in the area of the base of the alveolar process was associated with a decrease in the maximum values of equivalent stresses in implants by 16–63 %. In bone tissue, load reduction occurred by 30–53 % compared to the model where the bone graft was located along the lower edge of the jaw. Conclusions. With a higher location of the bone component of the fibula flap, adequate stress-strain state conditions and normal distribution of local loads occurred, which obviously determines a better prognosis of osseointegration, survival and functioning of dental implants.
сегментарний дефект кістки; нижня щелепа; дентальна імплантація; протезування; біомеханічні властивості; напружено-деформований стан
segmental bone defect; mandible; dental implantation; prosthetic treatment; biomechanical properties; stress-strain state
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Kang YF, Shan XF, Zhang L, Mao C, Wang Y, Zhang J, et al. Vascularized free fibular flap in oral and maxillofacial reconstruction: a 20-year experience at a single institution using 2640 flaps. J Craniofac Surg. 2023 Jul-Aug;34(5):1459-63. doi: 10.1097/SCS.0000000000009193. PMID: 36727753.
- Brown JS, Lowe D, Kanatas A, Schache A. Mandibular reconstruction with vascularized bone flaps: a systematic review over 25 years. Br J Oral Maxillofac Surg. 2017 Feb;55(2):113-26. doi: 10.1016/j.bjoms.2016.12.010. PMID: 28065645.
- Hidalgo DA, Rekow A. A review of 60 consecutive fibula free flap mandible reconstructions. Plast Reconstr Surg. 1995 Sep;96(3):585-96. PMID: 7638283.
- Sozzi D, Novelli G, Silva R, Connelly ST, Tartaglia GM. Implant rehabilitation in fibular free flap reconstruction: a retrospective study of cases at 1–18 years following surgery. J Craniomaxillofac Surg. 2017 Oct;45(10):1655-61. doi: 10.1016/j.jcms.2017.06.021. PMID: 28823690.
- Del Fabbro M, Testori T, Kekovic V, Goker F, Tumedei M, Wang HL. A systematic review of survival rates of osseointegrated implants in fully and partially edentulous patients following immediate loading. J Clin Med. 2019 Dec;8(12):2142. doi: 10.3390/jcm8122142. PMID: 31817177.
- Hidalgo DA. Fibula free flap mandible reconstruction. Microsurgery. 1994;15(4):238-44. doi: 10.1002/micr.1920150404. PMID: 8035668.
- Ong A, Williams F, Tokarz E, Shokri T, Hammer D, Ducic Y. Jaw in a day: immediate dental rehabilitation during fibula reconstruction of the mandible. Facial Plast Surg. 2021 Dec;37(6):722-7. doi: 10.1055/s-0041-1732478. PMID: 34380165.
- Gangwani P, Almana M, Barmak B, Kolokythas A. What Is the Success of Implants Placed in Fibula Flap? A Systematic Review and Meta-Analysis. J Oral Maxillofac Res. 2022 Mar 31;13(1):e3. doi: 10.5037/jomr.2022.13103. PMID: 35574211; PMCID: PMC9069636.
- Pavlychuk T, Chernogorskyi D, Chepurnyi Y, Neff A, Kop–chak A. Biomechanical evaluation of type p condylar head osteosynthesis using conventional small-fragment screws reinforced by a patient specific two-component plate. Head Face Med. 2020;16(1):25. doi: 10.1186/s13005-020-00236-0.
- Li X, Jiang C, Gao H, Wang C, Wang C, Ji P. Biomechanical analysis of various reconstructive methods for the mandibular body and ramus defect using a free vascularized fibula flap. Biomed Res Int. 2020;2020:8797493. doi: 10.1155/2020/8797493. PMID: 32258153.
- Mahardawi B, Jiaranuchart S, Damrongsirirat N, Arunjaroen–suk S, Mattheos N, Somboonsavatdee A, et al. The lack of keratinized mucosa as a risk factor for peri-implantitis: a systematic review and meta-–analysis. Sci Rep. 2023;13:3778. doi: 10.1038/s41598-023-30890-8.
- Tiwari A, Gupta VK, Haldkar RK, Parinov IA. Biomechanical analysis of patient-specific temporomandibular joint implant and comparison with natural intact jaw bone using finite element method. Appl Sci. 2022;12(6):3003. doi: 10.3390/app12063003.