
Международный эндокринологический журнал Том 19, №7, 2023
Вернуться к номеру
Ультразвукові та демографічний предиктори місцевого метастазування папілярного раку щитоподібної залози на доопераційному етапі: прогностична модель
Авторы: Ліщинський П.О., Товкай О.А.
Український науково-практичний центр ендокринної хірургії, трансплантації ендокринних органів і тканин МОЗ України, м. Київ, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
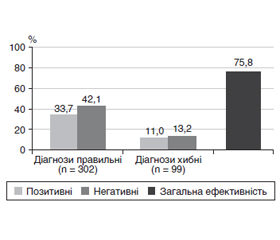
Актуальність. Через низьку чутливість і специфічність ультразвукового дослідження шиї при оцінці лімфатичних вузлів центрального колектора необхідно знайти альтернативні шляхи для прогнозування метастазів у центральні лімфатичні вузли шиї (CLNM) у пацієнтів з папілярним раком щитоподібної залози (ПРЩЗ). Мета: розробити прогностичну модель для оцінки ризику місцевого метастазування папілярного раку щитоподібної залози на основі доопераційних ультразвукових і демографічного предикторів. Матеріали та методи. Проведено ретроспективне моноцентрове когортне дослідження. Опрацьовано дані 401 пацієнта, яких було прооперовано з приводу ПРЩЗ. Основна група — 179 хворих, у яких виявлено CLNM на патогістологічному дослідженні (ПГД). Група порівняння — 222 пацієнти без метастазів за результатами ПГД. При проведенні аналізу враховувались як фактори ризику такі ознаки: субкапсулярне розташування пухлини; розмір; нечіткість меж; наявність ділянок кальцифікації (мікрокальцифікати); вік пацієнта. Критерії включення: цитологічно підтверджений ПРЩЗ на доопераційному етапі; оперовані пацієнти (тиреоїдектомія/гемітиреоїдектомія та центральна лімфатична дисекція шиї). Критерії виключення: операції в ділянці шиї у анамнезі; пацієнти з багатофокусним ураженням ЩЗ. Результати. За допомогою програми StatPlus було отримано таке логістичне рівняння: y = –1,839 – 0,037 × × X1 + 0,097 × X2 + 1,123 × X3 + 1,198 × X4 + 0,692 × X5, де X1, X2, X3, X4, X5 — вік (років), розмір (мм), субкапсулярне розташування (наявність), нечіткість меж (наявність), кальцифікати (наявність) відповідно. Отримана прогностична модель забезпечувала такі операційні характеристики при уточненні порогового значення для Р, яке дорівнює 0,44 (вирішальне правило X > T): чутливість — 75,4 %, специфічність — 79,3 %, діагностична ефективність — 75,1 %. З метою оцінки якості моделі було виконано процедуру ROC-аналізу. Отримані такі дані: площа під кривою (AUC) = 0,797 (95% ДІ: 0,753–0,841), що відповідає добрій якості моделі, індекс Юдена (J) = 0,5155. Перевірка якості моделі на контрольній групі зі 100 осіб дала такі результати: чутливість — 72,2 %, специфічність — 76,1 %, діагностична ефективність — 75,8 %. Висновки. Застосування математичної моделі на основі ультразвукових предикторів і віку пацієнта дає змогу прогнозувати наявність локальних метастазів ПРЩЗ на доопераційному етапі з діагностичною ефективністю 75,8 %. Жодна прогностична модель не дає 100% точності прогнозу. У виборі тактики лікування слід враховувати додаткові фактори впливу (опромінення в анамнезі, обтяжений сімейний анамнез тощо) на конкретного пацієнта.
Background. Due to the low sensitivity and specificity of neck ultrasound in the evaluation of the central lymph nodes, it is necessary to find alternative ways to predict central lymph node metastases in patients with papillary thyroid cancer (PTC). The purpose of the study is to develop a prognostic model for assessing the risk of local metastasis of papillary thyroid cancer based on preoperative ultrasound and demographic predictors. Materials and methods. A retrospective monocenter cohort study was conducted. The data of 401 patients who underwent surgery for PTC were processed. The main group included 179 patients in whom central lymph node metastases were detected during histopathological examination. The comparison group consisted of 222 patients without metastases according to the results of histopathological examination. When conducting the analysis, the following signs were considered as risk factors: subcapsular location of the tumor; size; blurred boundaries; the presence of calcification areas (microcalcifications); age of a patient. Inclusion criteria: PTC that was cytologically confirmed at the preoperative stage; surgeries (thyroidectomy/hemithyroidectomy and central neck lymph node dissection). Exclusion criteria: history of neck surgery; multifocal lesions of the thyroid gland. Results. The following logistic equation was obtained using the StatPlus program: y = –1.839 – 0.037 × X1 + 0.097 × X2 + 1.123 × X3 + 1.198 × X4 + + 0.692 × X5, where X1, X2, X3, X4, X5 are age (years), size (mm), subcapsular location (presence), blurred boundaries (presence), calcifications (presence), respectively. The obtained prognostic model provided the following operational characteristics when specifying the threshold value for P, which is equal to 0.44 (the decisive rule X > T): sensitivity — 75.4 %, specificity — 79.3 %, diagnostic efficiency — 75.1 %. To assess the quality of the model, the receiver operator characteristic (ROC) analysis was performed. The following data were obtained: area under the ROC curve = 0.797 (95% confidence interval: 0.753–0.841), which corresponds to the good quality of the model, and Youden index J = 0.5155. Checking the quality of the model on a control group of 100 people gave the following results: sensitivity — 72.2 %, specificity — 76.1 %, diagnostic efficiency — 75.8 %. Conclusions. The application of a prognostic model based on ultrasound data and the patient’s age makes it possible to predict the presence of local metastases of the PTC at the preoperative stage with a diagnostic efficiency of 75.8 %. No prognostic model gives 100% prediction accuracy. When choosing the treatment, additional influencing factors (history of radiation exposure, burdened family history, etc.) for a specific patient should be considered.
папілярний рак щитоподібної залози; фактори підвищення ризику метастазування; прогностична модель; лімфатичні вузли центрального колектора
papillary thyroid cancer; factors increasing the risk of metastasis; prognostic model; central lymph nodes
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Hu Q., Zhang W.J., Liang L., Li L.L., Yin W., Su Q.L., Lin F.F. Establishing a Predictive Nomogram for Cervical Lymph Node Metastasis in Patients With Papillary Thyroid Carcinoma. Front. Oncol. 2022 Jan 19. 11. 766650. doi: 10.3389/fonc.2021.766650. PMID: 35127475; PMCID: PMC8809373.
- Feng J.W., Ye J., Hong L.Z., Hu J., Wang F., Liu S.Y., –Jiang Y., Qu Z. Nomograms for the prediction of lateral lymph node metastasis in papillary thyroid carcinoma: Stratification by size. Front. Oncol. 2022 Sep 28. 12. 944414. doi: 10.3389/fonc.2022.944414. PMID: 36248990; PMCID: PMC9554485.
- Zhou S.C., Liu T.T., Zhou J., Huang Y.X., Guo Y., Yu J.H., Wang Y.Y., Chang C. An Ultrasound Radiomics Nomogram for Preope–rative Prediction of Central Neck Lymph Node Metastasis in Papillary Thyroid Carcinoma. Front. Oncol. 2020 Sep 4. 10. 1591. doi: 10.3389/fonc.2020.01591. PMID: 33014810; PMCID: PMC7498535.
- Wang M., Li R., Zou X., Wei T., Gong R., Zhu J., Li Z. A miRNA-clinicopathological nomogram for the prediction of central lymph node metastasis in papillary thyroid carcinoma-analysis from TCGA database. Medicine (Baltimore). 2020 Aug 28. 99(35). e21996. doi: 10.1097/MD.0000000000021996. PMID: 32871952; PMCID: PMC7458192.
- Wang Y., Guan Q., Xiang J. Nomogram for predicting level V lymph node metastases in papillary thyroid carcinoma with clinically lateral lymph node metastases: A large retrospective cohort study of 1037 patients from FDUSCC. J. Cancer. 2019 Jan 1. 10(3). 772-778. doi: 10.7150/jca.28527. PMID: 30719177; PMCID: PMC6360426.
- Sun F., Zou Y., Huang L., Shi Y., Liu J., Cui G., Zhang X., Xia S. Nomogram to Assess the Risk of Central Cervical Lymph Node Metastasis in Patients With Clinical N0 Papillary Thyroid Carcinoma. Endocr. Pract. 2021 Dec. 27(12). 1175-1182. doi: 10.1016/–j.eprac.2021.06.010. Epub 2021 Jun 24. PMID: 34174413.
- Tovkai O.A., Palamarchuk V.O., Lishchynskyi P.O., Kuts V.V., Stotska L.V., Chirkov Y.E., Zemskov S.V. Possibilities of ultrasound imaging in the detection of central lymph nodes metastases of papillary thyroid cancer. Clinical Endocrinology and Endocrine Surgery. 2020. 71(3). 7-15. DOI: https://doi.org/10.30978/CEES-2020-3-7 (in Ukrainian).
- Sun Y., Sun W., Xiang J., Zhang H. Nomogram for predicting central lymph node metastasis in T1-T2 papillary thyroid cancer with no lateral lymph node metastasis. Front. Endocrinol. (Lausanne). 2023 Jan 19. 14. 1112506. doi: 10.3389/fendo.2023.1112506. PMID: 36817601; PMCID: PMC9930606.
- Yang Z., Heng Y., Lin J., Lu C., Yu D., Tao L., Cai W. Nomogram for Predicting Central Lymph Node Metastasis in Papillary Thyroid Cancer: A Retrospective Cohort Study of Two Clinical Centers. Cancer. Res. Treat. 2020 Oct. 52(4). 1010-1018. doi: 10.4143/crt.2020.254. Epub 2020 Jun 9. PMID: 32599980; PMCID: PMC7577812.
- Hei H., Song Y., Qin J. Individual prediction of lateral neck metastasis risk in patients with unifocal papillary thyroid carcinoma. Eur. J. Surg. Oncol. 2019 Jun. 45(6). 1039-1045. doi: 10.1016/j.ejso.2019.02.016. Epub 2019 Feb 21. PMID: 30824213.
- Luisa Garo M., Deandreis D., Campennì A., Vrachimis A., Petranovic Ovcaricek P., Giovanella L. Accuracy of papillary thyroid cancer prognostic nomograms: a systematic review. Endocr. Connect. 2023 Mar 10. 12(4). e220457. doi: 10.1530/EC-22-0457. PMID: 36662681; PMCID: PMC10083677.
- Medas F., Canu G.L., Cappellacci F., Boi F., Lai M.L., Erdas E., Calò P.G. Predictive Factors of Lymph Node Metastasis in Patients With Papillary Microcarcinoma of the Thyroid: Retrospective Analysis on 293 Cases. Front. Endocrinol. (Lausanne). 2020 Aug 25. 11. 551. doi: 10.3389/fendo.2020.00551. PMID: 32982963; PMCID: PMC7477034.
- Xia E., Chi Y., Jin L., Shen Y., Hirachan S., Bhandari A., Wang O. Preoperative prediction of lymph node metastasis in patients with papillary thyroid carcinoma by an artificial intelligence algorithm. Am. J. Transl. Res. 2021 Jul 15. 13(7). 7695-7704. PMID: 34377246; PMCID: PMC8340231.
- Sahin S., Daglar G., Menekse E., Cavdarli B., Baglan T. The Effect of BRAF V600E Mutation on Lymph Node Involvement in Papillary Thyroid Cancer. Turk. J. Surg. 2020 Sep 28. 36(3). 249-255. doi: 10.47717/turkjsurg.2020.4696. PMID: 33778379; PMCID: PMC7963314.