
Журнал «Почки» Том 12, №1, 2023
Вернуться к номеру
Якість життя хворих з додіалізною хронічною хворобою нирок, її зв’язок з оксидантним стресом і екскрецією уромодуліну
Авторы: Денова Л.Д. (1), Іванов Д.Д. (2)
(1) — Національний університет охорони здоров’я імені П.Л. Шупика, м. Київ, Україна
(2) — Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
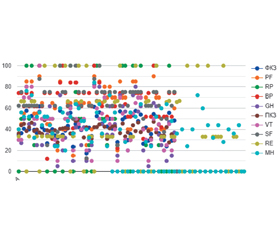
Метою роботи було оцінити якість життя (ЯЖ) пацієнтів з додіалізною хронічною хворобою нирок (ХХН), встановити фактори, що впливають на ЯЖ у даної категорії пацієнтів, і дослідити вплив антиоксидантної терапії на ЯЖ пацієнтів із ХХН 1–5-ї стадії. Матеріали та методи. У дослідженні взяли участь пацієнти із ХХН (n = 61), середній вік яких становив 44,51 ± 11,90 року. Двадцять (32,79 %) чоловіків і 41 (67,21 %) жінка були розподілені на дві групи, які були репрезентативними за віковим і гендерним складом: 1-ша група (n = 31) — пацієнти з ХХН, які 3 місяці приймали глутатіон по 100 мг 2 рази на добу під час їди, 2-га група (n = 30) — пацієнти з ХХН, які 3 місяці приймали убіхінон по 100 мг 1 раз на добу під час вживання їжі. ЯЖ оцінено за допомогою анкети SF-36. Прихильність пацієнтів до лікування визначали за допомогою анкети Моріскі — Гріна (MMAS-4). З метою оцінки функції нирок пацієнтів визначалися рівень екскреції уромодуліну сечі (uUMOD), співвідношення альбуміну й креатиніну сечі (САК). Оцінено вплив антиоксидантної терапії на ЯЖ даної категорії пацієнтів і встановлено фактори, що впливають на ЯЖ у даної категорії пацієнтів. Результати. У структурі ХХН переважала сечокам’яна хвороба — 22 особи (36,1 %), хворих на хронічний пієлонефрит було 5 осіб (8,2 %), діабетична нефропатія була у 18 пацієнтів (29,5 %), полікістоз нирок — у 4 хворих (6,6 %), подагрична нефропатія — у 6 (9,8 %), хронічний гломерулонефрит — в 1 (1,6 %), гіпертензивна нефропатія — у 5 хворих (8,2 %). Тривалість ХХН у першій групі становила 5,42 ± 3,88 (1; 15) року, у другій групі — 5,57 ± 3,79 (1; 16) року, вірогідної різниці між групами за віком і статтю не виявлено (U = 463m, р = 0,9827). У всіх пацієнтів на початку дослідження показники були меншими, ніж у кінці дослідження. Найнижчий показник в першій групі — «загальне здоров’я», у другій — «життєва активність». Психологічний компонент здоров’я (ПКЗ) був нижчим за фізичний компонент здоров’я (ФКЗ) в обох групах. Спостерігався значний позитивний зв’язок (p < 0,001), який був найбільше виражений щодо розрахункової швидкості клубочкової фільтрації (рШКФ), САК, систолічного артеріального тиску, гемоглобіну. У кінці дослідження 12 пацієнтів (19,67 %) мали 4 бали за шкалою Моріскі — Гріна, що означало високу прихильність до терапії. Було отримано вірогідний сильний позитивний зв’язок між ЯЖ і рШКФ, САК, uUMOD. На початку лікування між показником ЯЖ (ФКЗ) і uUMOD був значний середній позитивний зв’язок: r (59) = 0,372; p = 0,003, між показником ЯЖ (ФКЗ) і рШКФ — значний позитивний зв’язок: r (59) = 0,707; p < 0,001. Між показником ЯЖ (ПКЗ) і прихильністю пацієнтів до лікування існує дуже незначний позитивний зв’язок: r (59) = 0,0882, p = 0,499. Висновки. Антиоксидантна терапія глутатіоном і убіхіноном суттєво покращує ЯЖ пацієнтів із ХХН. Враховуючи безпеку й ефективність антиоксидантної терапії, ми пропонуємо включити антиоксидантну терапію в протоколи лікування пацієнтів із ХХН. Для опрацювання стандартного протоколу рекомендовано подальші дослідження.
Background. The purpose of this study was to assess the quality of life (QoL) in patients with pre-dialysis chronic kidney disease (CKD), to reveal the factors affecting the QoL in this category of patients and to investigate the effect of antioxidant therapy on the QoL of patients with CKD stages 1–5. Materials and methods. Patients with CKD (n = 61), whose average age was 44.51 ± 11.90 years, were included in the study. Twenty (32.79 %) men and 41 (67.21 %) women were divided into two groups representative in terms of age and gender composition: group 1 (n = 31) — patients with CKD who took glutathione 100 mg 2 times a day with meals for 3 months, group 2 (n = 30) — those with CKD who took ubiquinone 100 mg once daily with meals for 3 months. The QoL was assessed using the SF-36 questionnaire. Patient adherence to treatment was assessed with the Morisky-Green test. To assess the kidney function of patients, the level of urinary uromodulin excretion (uUMOD), urine albumin-to-creatinine ratio (ACR) were determined. The impact of antioxidant therapy on the QoL of these patients was evaluated and the factors affecting QoL were determined. Results. In the structure of CKD, urolithiasis was most common — 22 (36.1 %) patients, 5 (8.2 %) people had chronic pyelonephritis, 18 (29.5 %) — diabetic nephropathy, 4 (6.6 %) — polycystic kidney disease, 6 (9.8 %) — gouty nephropathy, 1 (1.6 %) — chronic glomerulonephritis and 5 (8.2 %) patients presented with hypertensive nephropathy. The duration of CKD in the first group was 5.42 ± 3.88 (1; 15) years, in the second one — 5.57 ± 3.79 (1; 16) years, no significant difference was found between the groups in terms of age and gender (U = 463m, p = 0.9827). In all patients, the indicators at the beginning were lower than those by the end of the study. The lowest indicator in the first group is general health, in the second — vitality. The psychological component of health (PsCH) was lower than the physical component of health (PhCH) in both groups. A significant positive relationship (p < 0.001) was observed, which was most pronounced for glomerular filtration rate (GFR), ACR, systolic blood pressure, hemoglobin. At the end of the study, 12 (19.67 %) patients had 4 points on the Morisky-Green test, which meant high adherence to therapy. There was a reliable strong positive relationship between the QoL and GFR, ACR, uUMOD. At the beginning of treatment, a significant average positive relationship was found between the QoL (PhCH) and uUMOD: r (59) = 0.372, p = 0.003; between the QoL (PhCH) and GFR, there is a significant positive relationship: r (59) = 0.707, p < 0.001. There is a very insignificant positive relationship between the QoL (PsCH) and patients’ adherence to treatment, r (59) = 0.0882, p = 0.499. Conclusions. Antioxidant therapy with glutathione and ubiquinone significantly improves the QoL of patients with CKD. Considering the safety and effectiveness of antioxidant therapy, we suggest including antioxidant therapy in treatment protocols for patients with CKD. Further research is recommended to determine a standard protocol.
хронічна хвороба нирок; глутатіон; убіхінон; антиоксидантна терапія; якість життя
chronic kidney disease; glutathione; ubiquinone; antioxidant therapy; quality of life