Резюме
Розсіяний склероз (РС) є найбільш відомим і поширеним по всій земній кулі демієлінізуючим захворюванням нервової системи. На РС хворіє близько 3 млн дорослого населення планети (приблизно 0,5–1‰) та близько 20 тис. в Україні. Це захворювання входить до числа так званих «чотирьох вершників неврологічного апокаліпсису» за своїми медичними й соціальними наслідками. Захворювання посідає друге місце за частотою в пацієнтів працездатного віку з інвалідизацією, супроводжується психо-емоційними змінами, що проявляються поведінковими порушеннями. Препарати патогенетичної і симптоматичної терапії дозволяють уповільнити прогресування хвороби, збільшити тривалість життя більшості хворих на РС. Проте є цілий ряд немоторних чинників, що змінюються під час захворювання, впливають на самосприйняття пацієнта, його професійні та соціальні якості. Такі люди часто схильні до депресії та тривожності, вони емоційно нестабільні та схильні до частих та різких перепадів настрою. Інтегральним показником фізичного, психологічного, емоційного й соціального функціонування хворого на РС є якість життя. У дослідженні оцінювали якість життя у хворих на РС з інвалідністю.
Рассеянный склероз (РС) является наиболее известным и распространенным по всему земному шару демиелинизирующим заболеванием нервной системы. РС болеет около 3 млн взрослого населения планеты (приблизительно 0,5–1 ‰) и около 20 тыс. в Украине. Данная патология входит в число так называемых «четырех всадников неврологического апокалипсиса» по своим медицинским и социальными последствиям. Заболевание занимает второе место по встречаемости среди пациентов трудоспособного возраста с инвалидизацией, сопровождается психоэмоциональными изменениями, которые проявляются поведенческими нарушениями. Препараты патогенетической и симптоматической терапии позволяют замедлить прогрессирование болезни, увеличить продолжительность жизни большинства больных РС. Однако есть целый ряд немоторных факторов, изменяющихся во время заболевания, которые влияют на самовосприятие пациента, его профессиональные и социальные качества. Такие люди часто склонны к депрессии и тревожности, они эмоционально нестабильны и подвержены частым и резким перепадам настроения. Интегральным показателем физического, психологического, эмоционального и социального функционирования больного РС является качество жизни. В исследовании оценивали качество жизни у больных РС с инвалидностью.
Multiple sclerosis (MS) is the best known and widespread demyelinating disease of the nervous system. About 3 million people suffer from MS in the world (about 0.5–1 ‰) and about 20,000 in Ukraine. It is among the “four horsemen of the neurological apocalypse” due to its medical and social implications. The disease ranks second among the disabled patients of working age and is accompanied by the acute neuropsychological changes, which manifest themselves in the abnormal behavior. The use of drugs of pathogenetic and symptomatic therapy, including the remedies that slow the progression of the disease, allows increasing the life expectancy of most patients with MS. However, there are several non-motor factors that change during the course of the disease, modifying the patient’s self-perception, professional, and social qualities. Such people are often prone to depression and anxiety, they are emotionally unstable and prone to frequent and sudden mood swings. An integral indicator of the physical, psychological, emotional, and social functioning of a patient with MS is the quality of life. The research provides an evaluation of the quality of life in MS patients with disability.
Introduction
Multiple sclerosis (MS) is the best known and widespread demyelinating disease of the nervous system [1]. About 3 million people suffer from MS in the world (about 0.5–1 ‰) and about 20,000 in Ukraine. It is among the “four horsemen of the neurological apocalypse” due to its medical and social implications [2]. The disease ranks se-cond among the disabled patients of working age and is accompanied by the acute neuropsychological changes, which manifest themselves in the abnormal behavior. The use of drugs of pathogenetic and symptomatic therapy, including the remedies that slow the disease progression, allows increasing the life expectancy of most patients with MS [3]. However, the study results demonstrate a limited influence of neurological impairment on the perceived quality of life, while age and depressive symptoms have a major influence [4, 5]. Moreover, there are several other non-motor factors that change during the course of the disease, modifying the patient’s self-perception, professional, and social qualities. People suffering from MS are often prone to depression and anxiety, they are emotionally unstable and prone to frequent and sudden mood swings. Researches inform that MS-associated fatigue and depression are common treatable features of MS, which could also impact the quality of life, irrespective of the physical disability [6, 7]. The reason for this wide range of cognitive impairments could be due to variations in the clinical backgrounds [8]. The patients need regular follow-up evaluations with a focus on non-motor problems and to be offered the best treatment available at that moment [9]. At the same time, the impact of treatment on the quality of life is poorly understood [10]. The evaluation of the quality of life, as an integral indicator of the physical, psychological, emotional, and social functioning of a patient with MS, gives a better understanding of causative factors that affect the physical and mental health of a patient with MS. Consequently, the studies have to emphasize newer MS management solutions that may have not reached their full potential yet [11].
Purpose of the study: evaluation of the quality of life in patients with MS with long-term pain syndrome/disability.
Materials and methods
The study was conducted at the Department of Neurology, I. Horbachevsky Ternopil National Medical University, based on the 1st, 2nd, 4th neurological departments of Ternopil Regional Municipal Neuropsychiatric Hospital in 2019–2020. Twenty-five patients (men — 11, women — 14) with MS were examined. The average age of the patients was 37 ± 17 years, the duration of the disease at the moment of the examination was 9.44 ± 10.56 years.
The clinical and neurological research methods were used to collect complaints, study the medical history, conduct objective examination to determine the neurological status. The diagnosis in patients with multiple sclerosis is reliable and established using international criteria (McDonald, 2005 and 2017) and is based on neuroimaging data (magnetic resonance imaging). The neurological deficit was established according to the Functional System scale; the degree of disability was determined by the Expanded Disability Status Scale (EDSS).
The classification of patients with MS was based on the clinical form, type of the course, stage, and duration of the disease, disability degree.
Depending on the type of the course, the patients with MS were divided into 3 groups. There were 18 patients with a relapsing-remitting course of MS, 4 with a primary progressive course, 3 with a secondary progressive course.
Twenty-one patients with a relapsing-remitting course were diagnosed with the acute stage of MS, 4 patients had a remission.
The degree of disability was assessed on the EDSS, which contains criteria for evaluating the visual, stem, pyramidal, cerebellar, sensory, pelvic function, brain function, and mobility of a patient. The assessment range is 10 points, where 0 means normal (no disability), 10 means death.
Disability of patients has 3 stages: mild (from 1 to 3.0 points), moderate (3.5–5.5 points), severe (over 6.0).
Analyzing possible risk factors, which accompany the beginning of the MS, it was found that most patients indicated the emotional stress and infection (influenza virus disease, Lyme disease, Botkin’s disease): in each of both groups, there were 7 (28 %) patients. Three (12 %) patients noticed the link with birth, 2 (8 %) patients — excessive physical work, and 2 (8 %) patients — traumatic brain injury. Four (16 %) MS patients denied the appearance of any factor, which preceded the onset of the disease.
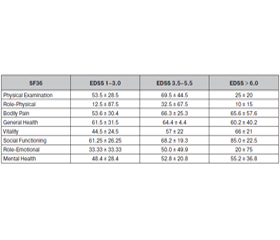
The quality of life was assessed by non-specific questionnaire Short Form 36 Health Survey (SF-36), which consists of 11 chapters, the result is shown in scores on 8 scales: General Health — evaluation of the patient’s general health state at the moment and during the treatment; Physical Functio-ning reflects the degree of influence of physical activity on the quality of life of the patient; Role-Physical — the impact of the physical condition on the quality of life, work performance or other daily activities; Role-Emotional — the impact of emotional state on the quality of life, work or other daily activities; Social Functioning — the influence of the physical or emotional state on the limitation of social activity; Bodily Pain — the pain intensity and its effect on the ability to engage in daily activities; Vitality — vital activity; Mental Health — self-assessment of mental health. Evaluation of each scale ranges between 0 and 100, where 100 means complete health. These scales form two indicators: physical component and the psychological component of health.
Statistical data processing was performed using the me-thods of variation statistics and correlation analysis. The SF-36 Health Survey Reference Kit statistical software package was used to process the SF-36 scales.
Anxiety and depression were assessed with the Hospital Anxiety and Depression Scale by Zigmond A.S., Snaith R.R. (HADS), where 0–7 points — normal status (lack of reliable symptoms of anxiety and depression), 8–10 — subclinical anxiety/depression, 11 points and more — clinically overt anxiety and depression.
Results and discussion
The comparison of the degree of disability of patients with MS and the physical component of the SF-36 scale (Table 1) demonstrated that the relationship between the investigated features is inverse, the strength of correlation on the Chaddock scale is noticeable, the correlation coefficient (r) is –0.629. At the same time, the results of the study of the EDSS index and the psychological component of the SF-36 showed that the correlation coefficient (r) was 0.162, the relationship between the studied traits was straight, and the strength of correlation on the Chaddock scale is weak.
/75.jpg)
Nine patients with subclinical manifestations of anxiety and depression on the HADS showed the following data: eight of them presented with mild disability by EDSS, one with the average degree of disability by EDSS. Two patients experienced clinically overt symptoms of anxiety and depression on the HADS, they both had a severe disability by EDSS. Statistically, the dependence is following: the correlation coefficient (r) is 0.913, the relationship between the studied traits is straight, the strength on the Chaddock scale is quite high, the Student’s t-test is 6.697, and the dependence of the traits is statistically significant (p < 0.001). Among 7 patients, citing the stress as a provoking factor of the disease, the subclinical manifestations of anxiety and depression were detected only in 2 individuals.
In patients with severe anxiety and depression (subclinical and clinical), the evaluation of the physical and psychological health component showed the following: between the HADS index and the physical health component of the SF-36 scale the correlation coefficient (r) is –0.597, the relationship between the studied traits is inverse, the strength of correlation on the Chaddock scale is noticeable. The correlation coefficient of the HADS index and the psychological component of health (r) is –0.213, the relationship between the studied traits is the opposite, the strength of correlation on the Chaddock scale is weak.
Conclusions
1. Disability is directly related to the physical dysfunction of a patient, but may not affect his mental status, including the role-functioning (maternity, family relationships, professional activities) that is caused mostly by the emotional state, social and vital activity.
2. The physical component of the quality of life significantly influences the neuropsychological status of patients, including the level of anxiety and depression. This can be explained by significant problems with self-care, daily routine, and physical work in patients with a high-degree disability on the EDSS, which significantly impairs self-esteem and proper perception of their condition.
3. Background stress, which is considered by patients to be a provoking factor for the development of the disease, is not a risk of anxiety and depression in the future. In opposite to previous, the severity of disability in most cases leads to psychological asthenization.
4. Thus, all parameters, which affect the quality of life of patients, can be divided into those, which can be modified and can’t be modified. Factors, which are modified, can be adjusted (for example, we can treat depression, asthenia, anxiety, improve the social adaptation of patients), thereby improving the quality of life of patients. Other factors, such as the gender of a patient, severity, and number of exacerbations of the disease per year, degree of disability, impact the patient’s quality of life to a lesser extent.
Conflicts of interests. Authors declare the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.
Список литературы
1. Ulitsky L.A., Chukhlovina M.L. Diagnosis of nervous diseases. 2001. P. 372.
2. Chuprina G.M. Multiple sclerosis: etiology, pathogenesis, clinic, diagnostics, differential diagnosis, treatment (clinical lecture). Eastern European Neurological Journal. 2017. 5. P. 27-37.
3. Sokolova L.I. Multiple sclerosis: key signs and treatments. III International Conference: Advances in Neurology. April 11–13, 2019.
4. Sharov D.A. Integral assessment of quality of life of patients with multiple sclerosis. Neuroimmunology. 2009. 1. P. 105-106.
5. Schwartz C.E., Foley F.W., Rao S.M., Bernardin L.J., Lee H., Genderson M.W. Stress and Course of Disease in Multiple Sclerosis. Behavioral Medicine. 1999. 25. 3. P. 110-116. doi: 10.1080/08964289909596740.
6. Janardhan V., Bakshi R. Quality of life in patients with multiple sclerosis: the impact of fatigue and depression. Journal of the neurological sciences. 2002. 205 (1). P. 51-58.
7. Beiske A.G., Svensson E., Sandanger I., Czujko B., Pedersen E.D., Aarseth J.H., Myhr K.M. Depression and Anxiety amongst Multiple Sclerosis Patients. European Journal of Neurology. 2008. 15. P. 239-245. doi: 10.1111/j.1468-1331.2007.02041.x.
8. Masaaki Niino, Yusei Miyazaki. Cognitive impairment as one of the important nonmotor symptoms in multiple sclerosis and neuromyelitis optica spectrum disorders. Clinical and Experimental Neuroimmunology. 2019. Vol. 10, Issue 3. doi: 10.1111/cen3.12528.
9. Beiske A.G. Non-motor symptoms in multiple sclerosis. Doctoral thesis, University of Oslo, 2009.
10. Gusev E.I., Boyko A.N. Multiple sclerosis: achievements of the decade. Journal of Neurology and Psychiatry. 2007. 4. P. 4-14.
11. Schmidt T.E. Pathogenetic treatment of multiple sclerosis. Medical Council. 2010. 9–10. P. 74-79.

/75.jpg)